How These Drugs Compare In Real Life
Sildenafil, tadalafil, and vardenafil belong to the same drug class: phosphodiesterase type 5 inhibitors, or PDE5 inhibitors. They help erections by enhancing the nitric oxide–cGMP pathway that relaxes penile smooth muscle and improves blood flow during sexual stimulation. That last part matters. None of these tablets creates an automatic erection on its own, and none of them increases libido. They improve the body’s erectile response when arousal is already there. Current urology guidance continues to treat PDE5 inhibitors as first-line oral therapy for most men with erectile dysfunction unless there is a contraindication.
That shared mechanism is why many people assume the three drugs are basically interchangeable. In practice, they are not. The most important differences are not mystical or brand-based. They are pharmacokinetic and practical: how quickly the drug tends to kick in, how long the useful window lasts, whether a heavy meal can blunt the effect, whether daily low-dose use is an option, and how side effects feel in ordinary life. Those variables often matter more to patient satisfaction than abstract efficacy percentages. A tablet that works well on paper may still disappoint if it does not fit the user’s timing, routines, or expectations.
Speed of Onset
For sildenafil, the usual useful rule of thumb is that it starts working in roughly 30 to 60 minutes, though the label notes peak blood concentrations may occur anywhere from 30 to 120 minutes, with a median around 60 minutes in the fasted state. The European Association of Urology guideline similarly describes a window of effectiveness beginning around 30 to 60 minutes after administration. That makes sildenafil workable for many men, but it is not a true “take it and go immediately” drug. It usually rewards a bit of planning.
Tadalafil can also begin to work from about 30 minutes after dosing, but its rhythm is different. The same guideline notes that peak efficacy is reached after about two hours, and the FDA-approved label reports a median time to maximum plasma concentration of about four hours. This does not mean tadalafil is “slow” in a useless sense. It means its onset can feel less tightly linked to one exact moment than sildenafil’s does. Some men experience that as freedom; others interpret it as less immediate feedback.
Vardenafil is often described as the most timing-sensitive contender for men who want a quicker start without moving to a different class altogether. The EAU guideline states that vardenafil is effective from 30 minutes after administration, and notes that about one in three patients may achieve satisfactory erections within 15 minutes. The FDA label places peak concentrations usually between 30 minutes and two hours, with a median around 60 minutes in the fasted state. In plain terms, vardenafil can feel a bit brisker for some users, though it is still not an “instant” pill.
This is where marketing often oversimplifies. The real-world difference in onset between these drugs is meaningful, but not absolute. A man who takes sildenafil correctly on an empty stomach and gives it enough time may find it perfectly reliable. Another man may repeatedly label sildenafil a failure simply because he took it after a large dinner and expected a response in 20 minutes. With PDE5 inhibitors, technique matters almost as much as molecule choice. That is one reason guidelines stress patient education and correct use rather than switching too quickly after one disappointing attempt.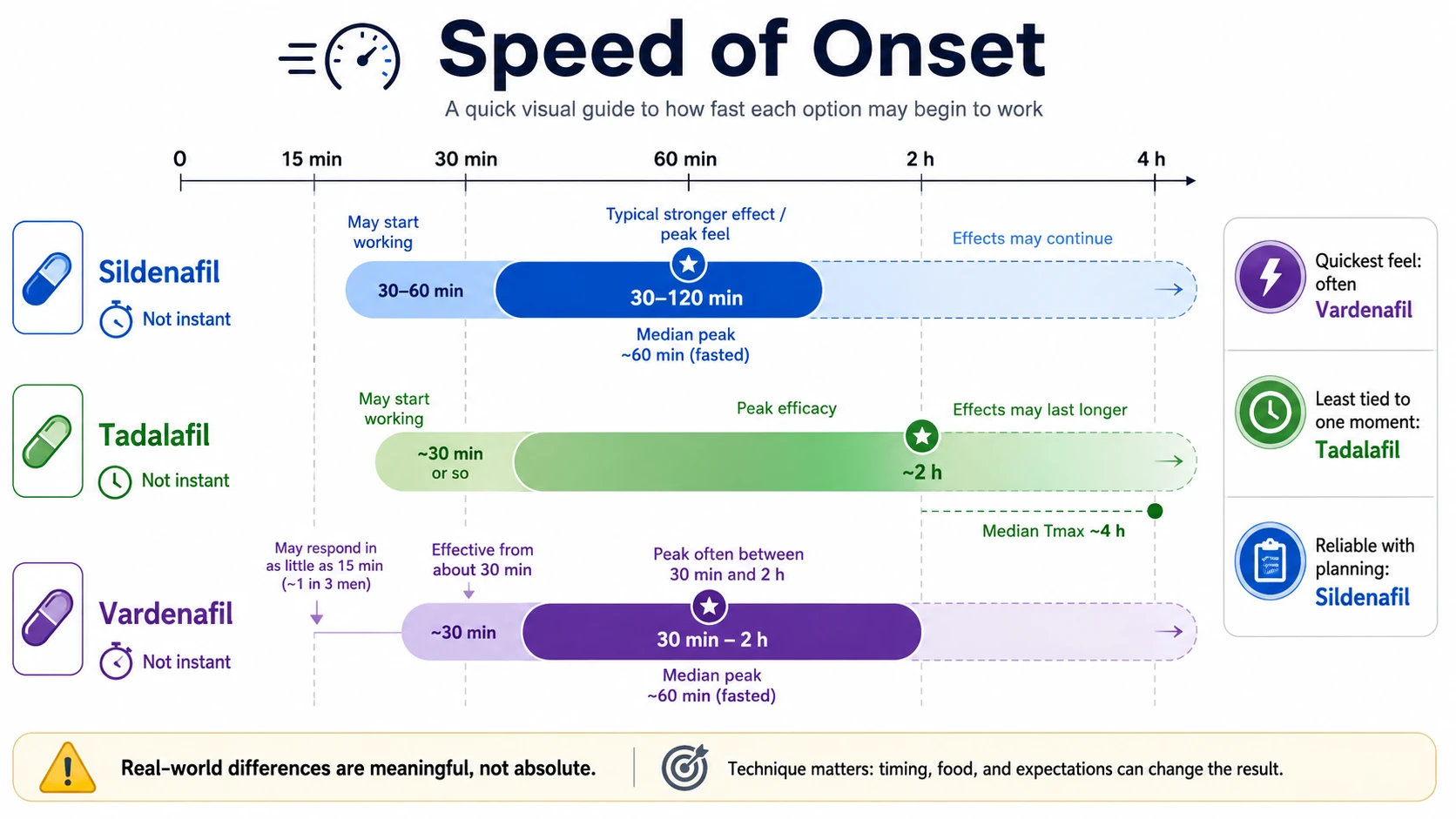
Duration of Effect
Duration is the point where tadalafil clearly separates itself from the other two. Sildenafil is usually thought of as a short-acting option. The EAU guideline gives a window of effectiveness from 30 to 60 minutes after dosing up to 12 hours, but in ordinary patient conversation it is still best understood as a medication with a much shorter practical sexual window than tadalafil. Many men experience it as a same-evening drug rather than an all-weekend one. That more limited window can actually be a benefit for users who prefer a more defined beginning and end to the effect.
Vardenafil is broadly similar to sildenafil in this respect. It is also an on-demand drug rather than a long-haul one. For buyers comparing labels and forum posts, vardenafil often lands in the middle psychologically: faster-feeling than tadalafil, but not dramatically longer-lived than sildenafil. It suits men who want an as-needed medication without carrying its effect deep into the next day.
Tadalafil is the outlier because its effect window can extend up to 36 hours. That does not mean a 36-hour erection, and it is important to say this plainly because many nonmedical descriptions still blur the point. What tadalafil provides is a prolonged period of improved erectile responsiveness. If sexual stimulation occurs within that window, the body may respond more easily. This long half-life is the reason tadalafil is commonly nicknamed the “weekend pill,” and also the reason many patients perceive it as the most natural-feeling option when spontaneity matters. Long duration has two opposite consequences. On the positive side, it reduces pressure. Men who become tense around the need to “perform on schedule” may feel less trapped by the clock when tadalafil is on board. The couple does not have to synchronize sex with one narrow pharmacologic peak. On the negative side, if side effects occur, they may also feel more prolonged. A headache or backache attached to tadalafil can linger longer than a similar problem with a shorter-acting drug, simply because the drug itself remains in the system longer.
There is also a subtler issue here. Some buyers think longer duration automatically means stronger efficacy. However, it does not. Duration answers the question “for how long might responsiveness be improved,” not “which drug is best for everyone.” A man who has infrequent, clearly planned sexual activity may not benefit much from a 36-hour window and may prefer the cleaner rhythm of sildenafil or vardenafil. Another man may find that the very existence of a narrow window worsens his anxiety and makes tadalafil a better psychological fit.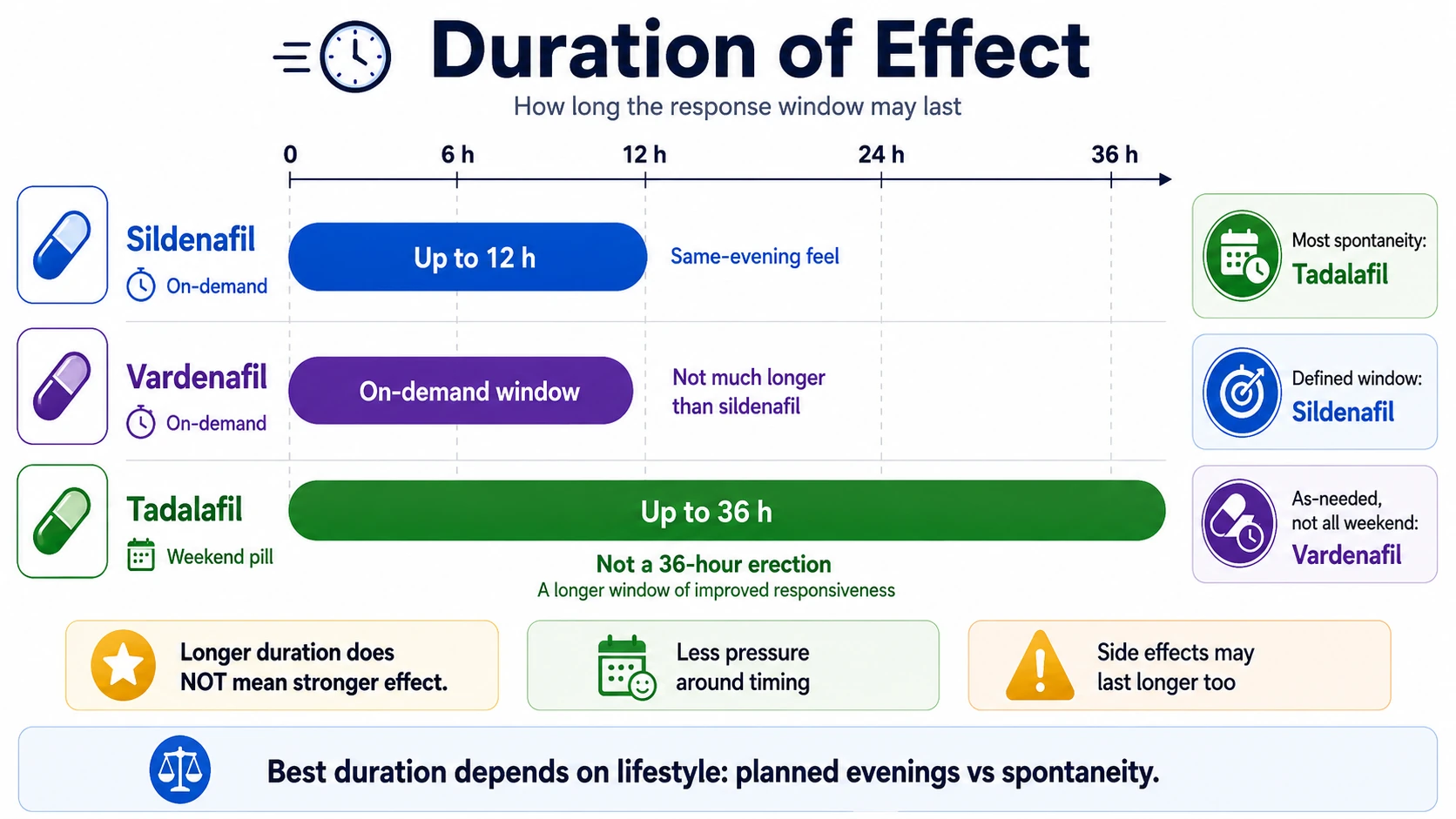
How They Are Taken
Sildenafil is usually started at 50 mg and adjusted up or down depending on effect and tolerability. The EAU guideline lists 25, 50, and 100 mg doses, with 50 mg as the usual starting point. It is taken on demand, typically before anticipated sexual activity rather than as a standing daily routine in standard ED use. That simple as-needed model is part of sildenafil’s appeal: it is familiar, widely available in generic form, and straightforward for first-time users.
Tadalafil offers something the others do not in routine practice: both on-demand and once-daily dosing. The guideline describes on-demand 10 and 20 mg dosing, usually starting at 10 mg, but it also allows 5 mg once daily for selected patients. Daily tadalafil changes the experience of treatment. Instead of linking every sexual encounter to a tablet taken shortly beforehand, it creates a background state in which sexual activity can be more spontaneous. This is not inherently superior, but it is a very different proposition.
Vardenafil is taken on demand, usually starting at 10 mg, with adjustment to 5 or 20 mg depending on response and tolerance. Like sildenafil, it fits a planned-use model. Its appeal is often to men who want an as-needed option but either did not love sildenafil’s performance in their own case or prefer vardenafil’s timing profile. It also exists in orally disintegrating formulations in some markets, which can matter to users who dislike swallowing tablets, although that does not automatically make it clinically stronger.
One practical issue many patients underestimate is that these medications sometimes need more than one properly conducted trial. Failure on attempt number one does not always mean the drug is wrong. The dose may be too low, the timing may be off, the meal may have interfered, alcohol may have dulled the response, or anxiety may have dominated the situation. In routine care, a clinician will often ask not “Did it work once?” but “How exactly did you take it, and under what circumstances?”
| Medication | How it is taken | Typical starting dose | Dose range | Best visual takeaway |
|---|---|---|---|---|
|
Sildenafil On-demand |
Before anticipated sexual activity | 50 mg | 25 / 50 / 100 mg | Simple, familiar, planned-use option |
|
Tadalafil On-demand or daily |
Either before sex or once daily | 10 mg on-demand 5 mg daily |
10 / 20 mg on-demand 5 mg daily |
Best fit for more spontaneous use |
|
Vardenafil On-demand |
Before anticipated sexual activity | 10 mg | 5 / 10 / 20 mg | Planned-use option; ODT exists in some markets |
Food, Alcohol, and Everyday Logistics
Food is one of the biggest real-life dividing lines among these drugs. Sildenafil is meaningfully affected by a high-fat meal. According to the DailyMed label, a fatty meal reduces the rate of absorption, delays time to peak by about 60 minutes, and lowers peak concentration. The practical translation is simple: sildenafil taken after a heavy dinner may still work, but often later and less cleanly than expected. For men who associate sex with restaurant meals, date nights, or late-evening indulgence, that matters a lot.
Vardenafil has a similar vulnerability. DailyMed notes that high-fat meals can reduce peak concentration by roughly 18% to 50% in food-effect studies. Again, the clinical takeaway is not that the tablet becomes useless, but that it may become less predictable. For a buyer choosing between molecules, this is one reason tadalafil often looks more forgiving in ordinary life. Tadalafil, by contrast, may be taken without regard to food. Its absorption is not meaningfully influenced by meals according to the FDA-approved labeling. That is a major convenience advantage, and not just a minor pharmacology footnote. It means tadalafil fits more easily into situations where sex is not separated from dinner, travel, alcohol, and irregular schedules. Many men do not need maximum theoretical potency. They need fewer ways to accidentally sabotage the dose.
Alcohol deserves a realistic mention too. None of these tablets cancels out the physiologic and behavioral effects of drinking. Heavy alcohol intake can worsen erectile performance on its own, lower blood pressure, and muddy the user’s ability to judge whether the drug is helping. Men sometimes conclude that a medication “failed,” when in fact the combination of fatigue, alcohol, stress, and poor timing overwhelmed the benefit. That does not make the drug bad; it means the context was hostile.
Side Effects and Safety Differences
The class side effects are familiar: headache, flushing, nasal congestion, dyspepsia, and dizziness. Across modern reviews, the overall efficacy and toxicity profiles of sildenafil, tadalafil, and vardenafil are broadly similar, with adverse events usually mild. That said, similarity does not mean sameness. Particular side effects cluster more with certain drugs, and those differences often shape preference more than efficacy tables do.
Sildenafil is the one most classically associated with transient visual adverse effects. That is related to off-target PDE6 activity and is one reason some men describe a blue tinge, altered color perception, or unusual light sensitivity. Not everyone gets this, and many users never notice it at all, but when it does occur it can be distinctive enough to push a switch to another PDE5 inhibitor.
Tadalafil is more often linked with back pain and myalgia. That does not mean the drug is rougher overall; many men tolerate it very well. But when muscle or lower-back discomfort occurs after tadalafil, it is a known pattern rather than a bizarre one-off. For some users that side-effect trade-off is worth the long duration and meal flexibility. For others, especially if musculoskeletal symptoms are already a nuisance, a shorter-acting alternative may feel cleaner.
Vardenafil tends to sit between the two in public perception, but it has one caution worth remembering: patients with congenital QT prolongation, or those taking certain class IA or III antiarrhythmics, are generally advised to avoid it. That does not make vardenafil unsafe for the average user, but it is one reason medication choice should not be reduced to online price comparisons alone. The “best” tablet depends partly on the cardiovascular and medication background, not just on sex timing.
All three share an absolute contraindication with nitrates because they can markedly potentiate hypotension through the nitric oxide–cGMP pathway. That point is nonnegotiable. They also require care with certain antihypertensives, alpha-blockers, and other interacting drugs. In addition, erectile dysfunction itself can be a marker of broader cardiometabolic disease, so self-prescribing from dubious online sources is risky for more reasons than fake pills alone. A proper ED assessment is part of identifying who can use these drugs safely and who needs a wider work-up.
What Buyers Usually Care About
Most buyers do not ask, “Which PDE5 inhibitor has the most elegant pharmacokinetic profile?” They ask some version of four simpler questions. How fast will it work. How long will it last. Can I take it after dinner. And how likely is it to make me feel strange. Those are sensible questions, because they reflect actual use rather than textbook classification. Price and familiarity often push first-time buyers toward sildenafil. It has been around longest, has strong name recognition, and is available generically in many markets. Clinically, that is not irrational. Sildenafil remains a perfectly valid starting option, especially for men who want on-demand use, have fairly predictable timing, and do not mind taking the tablet on a relatively empty stomach.
Tadalafil tends to attract buyers who dislike scheduling sex around a countdown clock. It is often the easiest drug to fit around meals, weekends away, spontaneous intimacy, and repeated attempts over a longer period. Men with performance anxiety about “having one chance” may prefer tadalafil precisely because it makes the encounter feel less pharmacologically staged. That does not mean it treats the psychological component directly, but it can reduce one trigger for it.
Vardenafil is often chosen by men looking for an on-demand drug that feels a little sharper or faster than sildenafil, or by those who simply did not get the desired result with sildenafil despite using it correctly. Response variability between patients is real. Two men with apparently similar erectile dysfunction may still prefer different agents because their timing, side-effect sensitivity, and subjective experience differ. The molecule that fits one couple’s rhythm may be the wrong one for another.
One point worth emphasizing for a buyer-oriented article is that “works best” is often a composite of medicine and circumstances. A tablet that gives a slightly firmer response but requires fasting, precise timing, and a narrow sexual window may be worse in practice than one that is marginally less dramatic but much easier to use consistently. Reliability is not only pharmacology. It is usability.
Who Should Lean Toward Which
Sildenafil is often the most logical first try for men who are new to ED medication, cost-conscious, and comfortable with some planning. It makes particular sense when sexual activity is reasonably predictable and the user can avoid taking it immediately after a heavy meal. It is also a reasonable choice for men who prefer a shorter active window and do not want to feel medicated into the next day. Check prices and terms for buying generic sildenafil
Tadalafil is often the best fit when spontaneity matters, when meals and travel make timing messy, or when performance pressure is amplified by the need to “hit the window.” It also deserves consideration when sexual activity is frequent enough that once-daily dosing seems attractive. In men who also have lower urinary tract symptoms associated with benign prostatic hyperplasia, tadalafil has an additional practical edge because guideline-level evidence supports its use in that overlap setting. Check prices and terms for buying generic tadalafil
Vardenafil can be a strong option for men who want an on-demand tablet, care about reasonably brisk onset, and either did not respond well to sildenafil or simply found it less suitable in their own routine. It is not the universally superior middle ground, but it is a legitimate alternative rather than an afterthought. The main caveat is that its cardiac and drug-interaction context should be reviewed carefully, particularly where QT issues or interacting medicines are in the picture. Check prices and terms for buying generic vardenafil
Conclusion
Sildenafil, tadalafil, and vardenafil all belong to the same therapeutic family, but they do not feel the same in use. Sildenafil is the classic planned option. Tadalafil is the least meal-sensitive and the longest-lasting, which makes it attractive for spontaneity and, in some patients, daily use. Vardenafil remains a credible on-demand alternative with a potentially brisk onset for the right user. The best choice is usually not the one with the loudest reputation, but the one whose timing, duration, food tolerance, side-effect pattern, and safety profile fit the patient’s real life.
References
- American Urological Association. (2018). Erectile dysfunction: AUA guideline. https://www.auanet.org/guidelines-and-quality/guidelines/erectile-dysfunction-%28ed%29-guideline
- Ala, C., Beley, S., Droupy, S., Giuliano, F., Loison, G., de la Taille, A., & Chevret-Méasson, M. (2025). Oral drug treatments of erectile dysfunction: AFU/SFMS guidelines overview. Progrès en Urologie. https://pubmed.ncbi.nlm.nih.gov/40915356/
- European Association of Urology. (2025). EAU guidelines on sexual and reproductive health: Management of erectile dysfunction. https://uroweb.org/guidelines/sexual-and-reproductive-health/chapter/management-of-erectile-dysfunction