GLP-1 receptor agonists: Dual systems of care in 2026
GLP-1 receptor agonists have undergone one of the most significant identity shifts in modern pharmacotherapy. Originally developed and positioned as treatments for type 2 diabetes, these agents are now equally associated with weight management, reshaping how clinicians, patients, and pharmacies understand metabolic disease. What was once a relatively contained therapeutic class within endocrinology has expanded into a dual-purpose platform that operates across two distinct clinical domains.
At a molecular level, nothing fundamental has changed. The same pathways are being targeted, the same receptors activated, and in many cases the same drugs are being used. Yet the context in which these therapies are prescribed has diverged sharply. In diabetes care, GLP-1 drugs remain part of a structured, guideline-driven approach focused on glycemic control and long-term complication prevention. In obesity care, the same agents are framed around weight reduction, cardiometabolic risk improvement, and, increasingly, quality of life. This divergence has created two parallel realities. Patients may receive similar medications but encounter very different expectations, access pathways, and treatment experiences. Pharmacies process the same molecules under different reimbursement rules and counseling frameworks. Clinicians apply different decision-making logics depending on indication. The result is not one therapeutic system, but two overlapping systems built on the same pharmacological foundation.
Understanding what is changing requires moving beyond the drug itself and examining how its meaning shifts depending on why it is prescribed.
Mechanism and Indications: Same Biology, Different Goals
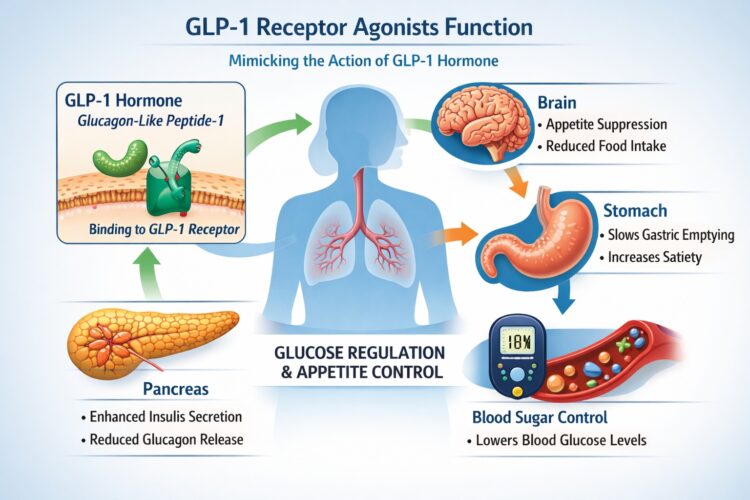 GLP-1 receptor agonists function through a well-characterized physiological pathway. They mimic the action of endogenous glucagon-like peptide 1, a hormone involved in glucose regulation and appetite control. By activating GLP-1 receptors, these drugs enhance glucose-dependent insulin secretion, suppress glucagon release, slow gastric emptying, and influence central appetite signaling. The result is a combination of improved glycemic control and reduced caloric intake. From a mechanistic standpoint, this dual action explains why the same class can be used for both diabetes and weight management. In type 2 diabetes, the primary therapeutic objective is to reduce blood glucose levels and lower HbA1c. The insulinotropic and glucagon-suppressing effects of GLP-1 agonists directly address these goals, making them an established component of diabetes treatment algorithms. Additional benefits, such as modest weight loss and cardiovascular risk reduction, are considered valuable but historically secondary.
GLP-1 receptor agonists function through a well-characterized physiological pathway. They mimic the action of endogenous glucagon-like peptide 1, a hormone involved in glucose regulation and appetite control. By activating GLP-1 receptors, these drugs enhance glucose-dependent insulin secretion, suppress glucagon release, slow gastric emptying, and influence central appetite signaling. The result is a combination of improved glycemic control and reduced caloric intake. From a mechanistic standpoint, this dual action explains why the same class can be used for both diabetes and weight management. In type 2 diabetes, the primary therapeutic objective is to reduce blood glucose levels and lower HbA1c. The insulinotropic and glucagon-suppressing effects of GLP-1 agonists directly address these goals, making them an established component of diabetes treatment algorithms. Additional benefits, such as modest weight loss and cardiovascular risk reduction, are considered valuable but historically secondary.
In obesity treatment, the hierarchy of outcomes is reversed. The appetite-regulating effects and impact on energy balance become the central focus. Weight loss is not a side effect but the primary endpoint. Clinical trials are designed around percent body weight reduction, achievement of predefined thresholds such as 10 or 15 percent loss, and improvements in obesity-related comorbidities. Glycemic effects remain relevant, particularly in patients with prediabetes or insulin resistance, but they are no longer the defining measure of success.
This shift in endpoints reflects a broader reframing of obesity as a chronic disease rather than a lifestyle issue. GLP-1 therapies are positioned as long-term treatments that modify biological drivers of weight, not short-term aids for dieting. That conceptual shift has profound implications for how these drugs are prescribed, evaluated, and reimbursed.
Indication-specific labeling reinforces this divergence. The same molecule may exist in different branded forms, each with its own approved use, dosing range, and clinical narrative. Semaglutide, for example, is used at lower doses for diabetes management and at higher doses for weight loss. Tirzepatide follows a similar pattern, with indications spanning glycemic control and obesity treatment. These distinctions are not merely administrative. They shape how clinicians initiate therapy, how insurers assess coverage, and how patients perceive the purpose of the medication. Another important difference lies in the interpretation of risk and benefit. In diabetes care, GLP-1 receptor agonists are often evaluated within a framework that prioritizes prevention of complications such as cardiovascular disease, nephropathy, and retinopathy. In obesity care, the benefits are framed more broadly, encompassing improvements in mobility, sleep, metabolic health, and overall well-being. This broader framing can make the value of treatment more visible to patients, but it also introduces variability in how success is defined.
The shared biology of GLP-1 therapies therefore masks a deeper divergence. The same mechanism is being deployed toward different clinical ends, and those ends influence everything from trial design to patient expectations. In diabetes, the drug is part of a tightly regulated metabolic control strategy. In obesity, it becomes a tool for sustained weight reduction and systemic health improvement.
This distinction is central to understanding the current landscape. It explains why two patients taking similar medications may have entirely different treatment journeys, and why the expansion of GLP-1 use has created both opportunities and tensions within healthcare systems.
From Endocrinology to Obesity Medicine: A Shift in Prescribing Authority
The expansion of GLP-1 therapies into weight management has not only changed what these drugs are used for, but also who is prescribing them and under what clinical framework. Historically, GLP-1 receptor agonists were firmly embedded within endocrinology. Their use was guided by diabetes-specific protocols, specialist oversight, and structured escalation pathways tied to glycemic targets. Prescribing authority was relatively concentrated, and decision-making followed established clinical algorithms. That model is now being disrupted. As GLP-1 therapies gained approval for obesity, prescribing began to diffuse beyond endocrinology into primary care, obesity medicine, and digital health platforms. General practitioners are increasingly initiating these therapies, often in response to patient demand or as part of broader cardiometabolic risk management. At the same time, a new ecosystem of weight management clinics has emerged, many of which specialize in pharmacologic obesity treatment and operate with a different clinical emphasis.
This shift reflects a deeper transformation. Obesity is no longer treated as a secondary concern within other specialties. It is becoming a primary therapeutic focus, with its own clinical pathways, patient populations, and treatment goals. GLP-1 drugs are at the center of this transition, acting as a bridge between traditional metabolic care and newer, more patient-driven models. Telehealth has accelerated this redistribution of prescribing authority. Digital platforms now offer structured consultations, remote monitoring, and medication management for obesity treatment. In these settings, GLP-1 therapies are often positioned as part of a broader service package that includes coaching, lifestyle guidance, and ongoing support. This contrasts with traditional diabetes care, where prescribing is typically embedded in a long-term physician-patient relationship within a defined healthcare system.
However, the decentralization of prescribing also introduces variability. Clinical rigor is not uniform across all providers. While many practitioners follow evidence-based protocols, others may rely on simplified or accelerated pathways that do not fully replicate the safeguards of specialist care. This raises important questions about consistency, safety, and the appropriate boundaries of digital prescribing.
Another consequence of this shift is the changing role of clinical expertise. In diabetes care, endocrinologists bring deep knowledge of insulin dynamics, complication management, and complex pharmacotherapy. In obesity medicine, the emphasis expands to include behavioral factors, long-term adherence, and patient motivation. These differences influence how GLP-1 therapies are introduced, titrated, and supported over time.
Importantly, patients themselves are shaping this evolution. Demand for weight loss treatments has surged, driven by increased awareness, social visibility, and the perceived effectiveness of GLP-1 drugs. Patients are no longer passive recipients of care. They actively seek out providers, compare options, and, in many cases, drive prescribing decisions through informed demand. This creates a feedback loop. As more providers enter the space, access expands. As access expands, demand grows further. The result is a prescribing environment that is more dynamic, more distributed, and less tightly controlled than the traditional diabetes model.
For pharmacies, this shift is immediately visible. Prescriptions are arriving from a wider range of providers, including telehealth services and specialized clinics that may operate across multiple jurisdictions. Verifying prescriber legitimacy, ensuring appropriate documentation, and maintaining consistent dispensing standards becomes more complex in this environment.
In 2026, GLP-1 prescribing is no longer confined to a single specialty. It has become a cross-disciplinary practice, shaped by clinical innovation, patient demand, and the rapid expansion of digital healthcare. This transformation is redefining not only who prescribes these drugs, but how they are integrated into broader models of care.
Dosing, Formulations, and Treatment Expectations
While the underlying molecules may be similar, dosing strategies and treatment expectations differ significantly between diabetes and weight loss indications. These differences are not merely technical. They shape patient experience, influence adherence, and alter how both clinicians and pharmacies approach therapy.
In diabetes care, GLP-1 receptor agonists are typically introduced as part of a stepwise treatment strategy. Doses are titrated gradually to balance glycemic control with tolerability. The primary goal is stabilization. Once an effective dose is reached and HbA1c targets are met, the focus shifts to maintenance. The therapy becomes part of a broader regimen that may include other medications, lifestyle interventions, and regular monitoring.
In obesity treatment, the trajectory is more dynamic. Dose escalation is still gradual, but the endpoint is different. The goal is not simply to reach a stable dose, but to achieve and sustain clinically meaningful weight loss over time. This often involves higher target doses compared to diabetes indications, reflecting the need for stronger appetite suppression and metabolic effects.
These higher doses can amplify both efficacy and side effects. Patients may experience more pronounced gastrointestinal symptoms during titration, which can influence their willingness to continue treatment. At the same time, the visible nature of weight loss can reinforce adherence, at least in the early stages. This creates a tension between therapeutic intensity and tolerability that is less pronounced in diabetes care. Formulation also plays a role. Injectable therapies remain the standard for both indications, but patient expectations differ. In diabetes, injections are often accepted as part of long-term disease management. In obesity treatment, especially among patients without prior experience with injectable drugs, there may be greater resistance or hesitation. This has driven interest in oral formulations and alternative delivery systems, which are seen as potential solutions to improve accessibility and adherence.
Treatment duration is another point of divergence. Diabetes therapies are generally understood to be lifelong, with adjustments over time. In obesity care, expectations are still evolving. Some patients approach GLP-1 therapy as a temporary intervention, aiming to achieve a target weight before discontinuing treatment. However, emerging evidence suggests that stopping therapy often leads to weight regain, reinforcing the concept of obesity as a chronic condition requiring ongoing pharmacologic support.
This mismatch between patient expectations and clinical reality can create challenges. Patients who view treatment as short-term may be less prepared for the long-term commitment required to maintain results. Clinicians must navigate these expectations carefully, balancing optimism with realistic guidance.
For pharmacies, these differences translate into distinct dispensing patterns. Diabetes prescriptions may be more stable and predictable, while obesity-related prescriptions can involve more frequent dose adjustments, therapy initiation, and discontinuation. Counseling also differs. In diabetes, the emphasis may be on glycemic monitoring and integration with other medications. In obesity, discussions often focus on side effects, weight trajectories, and the importance of persistence.
Ultimately, dosing and formulation are not just pharmacological details. They are central to how patients experience GLP-1 therapy and how successfully they remain on treatment. The divergence between diabetes and weight loss use becomes particularly visible at this level, where clinical strategy meets everyday practice.
Access, Coverage, and Reimbursement Divide
If mechanism defines what GLP-1 drugs can do, and dosing defines how they are used, coverage determines whether patients can access them at all. This is where the divergence between diabetes and obesity indications becomes most pronounced and most consequential.
In diabetes care, GLP-1 receptor agonists are widely integrated into treatment guidelines and reimbursement systems. They are recognized as effective therapies for glycemic control, with additional benefits in weight reduction and cardiovascular risk. As a result, most public and private insurance plans include them in formularies, often with manageable prior authorization requirements. While access is not entirely frictionless, it is generally predictable and structured. In obesity care, the situation is fundamentally different. Despite strong clinical evidence supporting the effectiveness of GLP-1 therapies for weight loss, coverage remains inconsistent and often restrictive. Many insurance plans explicitly exclude anti-obesity medications, classifying them as non-essential or lifestyle-related treatments. Where coverage does exist, it is frequently accompanied by strict criteria, including body mass index thresholds, documentation of failed lifestyle interventions, and repeated prior authorization processes.
This creates a paradox. The same drug, prescribed for diabetes, is treated as medically necessary and reimbursable. Prescribed for obesity, it may be considered optional or even discretionary. The molecule does not change, but its economic status does.
For patients, the implications are immediate and tangible. Out-of-pocket costs for GLP-1 therapies can be substantial, often exceeding what many individuals can sustain over time. Even patients who initially access treatment through coverage may face interruptions if policies change, if prior authorizations are denied, or if employers revise benefits. This instability undermines continuity of care and directly impacts outcomes.
Prior authorization itself has become a significant barrier. Clinicians must navigate administrative processes that require detailed documentation, justification, and, in some cases, repeated submissions. These processes consume time and resources, and they can delay treatment initiation. For patients, delays translate into frustration, disengagement, and, in some cases, abandonment of therapy. Employer-sponsored plans add another layer of complexity. Some employers have begun to include obesity medications as part of wellness initiatives, recognizing their potential to reduce long-term healthcare costs. Others have moved in the opposite direction, limiting coverage due to budget concerns. This variability means that access is often determined not by clinical need, but by the design of a specific benefits package.
There is also a growing distinction between indications within coverage frameworks. GLP-1 therapies with additional approved indications, such as cardiovascular risk reduction, may be more likely to receive reimbursement. This creates a situation in which patients with certain comorbidities have access, while others with similar weight-related risks do not. The result is a fragmented system where eligibility depends on diagnostic categorization as much as on clinical reality.
Pharmacies are directly affected by these dynamics. Processing GLP-1 prescriptions for obesity often involves more complex interactions with insurers, including verification of coverage, handling of denials, and communication with prescribers. Pharmacists may spend significant time assisting patients in navigating these barriers, explaining cost differences, and identifying alternative pathways.
The reimbursement divide also influences prescribing behavior. Clinicians may favor drugs that are more likely to be covered, even if they are not the first clinical choice. In some cases, this leads to therapeutic compromises, where treatment decisions are shaped by access rather than optimal efficacy.
In 2026, access is not a secondary consideration in GLP-1 therapy. It is a central determinant of who receives treatment, how long they stay on it, and what outcomes they achieve. The contrast between diabetes and obesity coverage highlights a broader tension within healthcare systems, where evidence-based therapies are not always matched by equitable access.
Adherence, Persistence, and Patient Experience
Even when patients overcome access barriers and initiate treatment, the next challenge is staying on therapy long enough to achieve meaningful and sustained outcomes. Adherence and persistence are where the divergence between diabetes and obesity use becomes most visible at the patient level.
In diabetes care, adherence is often driven by necessity. Patients are managing a condition with clear, measurable consequences. Blood glucose levels provide immediate feedback, and the risks of poor control are well understood. This creates a strong incentive to maintain treatment, even in the face of inconvenience or mild side effects. GLP-1 therapies are integrated into a broader regimen, and discontinuation is typically considered within the context of overall disease management.
In obesity treatment, adherence is more variable and often more fragile. Weight loss is a visible outcome, but it is not always linear or predictable. Patients may experience rapid initial progress followed by plateaus, which can affect motivation. Side effects, particularly gastrointestinal symptoms, can be more disruptive in individuals who are not accustomed to chronic medication use. The absence of immediate clinical markers comparable to blood glucose can make it harder to assess progress in a structured way.
Side effects remain one of the primary drivers of discontinuation. Nausea, vomiting, diarrhea, and constipation are common during dose escalation. While these effects are often temporary, they can be significant enough to lead patients to reduce doses, pause treatment, or stop altogether. The balance between efficacy and tolerability is therefore critical. A drug that produces greater average weight loss may not deliver better outcomes if it is less well tolerated by a specific patient. Psychological factors also play a role. Patients using GLP-1 therapies for weight loss often have different expectations and motivations compared to those using them for diabetes. Some may approach treatment with a short-term mindset, expecting to discontinue once a target weight is reached. Others may struggle with the idea of long-term pharmacologic support for weight management. These expectations can influence persistence and shape how patients respond to challenges during treatment.
There is also the issue of treatment fatigue. Weekly injections, ongoing monitoring, and the need to manage side effects can become burdensome over time. For some patients, this leads to gradual disengagement, even if the therapy is effective. In contrast, patients with diabetes may be more accustomed to long-term medication routines, making adherence more stable. Persistence is further affected by external factors such as cost and access. Interruptions in coverage, changes in insurance policies, or fluctuations in medication availability can disrupt treatment continuity. These disruptions can lead to cycles of initiation and discontinuation, reducing overall effectiveness and increasing the risk of weight regain.
For pharmacies, adherence challenges translate into irregular refill patterns, increased patient counseling needs, and more frequent interactions related to side effects and expectations. Pharmacists play a key role in supporting persistence, helping patients navigate tolerability issues, and reinforcing the importance of consistent use.
Ultimately, adherence is where clinical potential meets real-world behavior. The effectiveness of GLP-1 therapies depends not only on their pharmacological properties, but on the ability of patients to integrate them into their lives over the long term.
Pharmacy Operations: Workflow, Counseling, and Risk Management
For pharmacies, the rise of GLP-1 therapies has not been a simple increase in prescription volume. It has required a structural adaptation of workflows, verification processes, and patient communication strategies. The dual use of the same medications for diabetes and weight loss introduces operational complexity that did not exist when these drugs were confined to a single indication.
One of the most immediate changes is volume pressure. Demand for GLP-1 therapies has increased sharply, driven largely by obesity treatment. This has implications for inventory management, staffing, and dispensing timelines. Pharmacies must balance supply across patients using these drugs for diabetes and those using them for weight loss, often under conditions where availability, while improved compared to earlier shortages, is still uneven at the local level. Allocation decisions can become ethically and operationally sensitive, particularly when patients with chronic glycemic needs compete with new initiations for weight management. Verification processes have also become more complex. Prescriptions are now arriving from a broader range of sources, including traditional clinics, telehealth platforms, and specialized weight management services. Pharmacists must ensure that prescriptions are valid, that prescribers are appropriately licensed, and that documentation meets regulatory standards. This is especially important in the context of obesity treatment, where inappropriate prescribing practices have been a concern. The risk profile is not only clinical but also regulatory, requiring vigilance at the dispensing stage.
Counseling requirements differ depending on indication. For diabetes patients, counseling often focuses on glycemic monitoring, integration with other medications, and recognition of hypoglycemia risk in combination therapies. For weight loss patients, the emphasis shifts toward side effect management, expectations around weight trajectories, and the importance of adherence. Pharmacists must adapt their communication style and content accordingly, often within the same workflow.
There is also an increased need for patient education around dosing and titration. Because GLP-1 therapies involve gradual dose escalation, errors in administration can occur if patients misunderstand instructions. This risk is amplified when prescriptions are initiated through digital platforms, where in-person counseling may be limited.
Fraud prevention and misuse detection have become more prominent as well. The high demand and high cost of these medications create incentives for inappropriate prescribing, prescription diversion, or attempts to obtain medication without proper clinical evaluation. Pharmacists are positioned at a critical control point, where they can identify irregularities, verify legitimacy, and intervene when necessary. This role extends beyond dispensing into active risk management.
Operationally, GLP-1 therapies have also increased the administrative burden. Prior authorizations, insurance rejections, and coverage clarifications are more frequent for obesity indications. Pharmacy staff may spend significant time communicating with insurers and prescribers, explaining cost differences to patients, and identifying alternative options when coverage is denied.
Market and Regulatory Pressure: Where the System Is Moving
The rapid expansion of GLP-1 therapies has placed them at the center of market competition, regulatory scrutiny, and policy debate. What began as a therapeutic advance in diabetes has evolved into a broader transformation of how metabolic diseases are treated and understood.
Pharmaceutical competition is intensifying. Manufacturers are investing heavily in expanding indications, developing higher-dose formulations, and advancing next-generation compounds. The goal is not only to improve efficacy, but to differentiate products in a crowded and high-stakes market. New indications, such as cardiovascular risk reduction and obstructive sleep apnea, are redefining the value proposition of these drugs and influencing both prescribing patterns and reimbursement decisions.
Regulators are responding to this expansion with increased oversight. The widespread use of GLP-1 therapies, particularly in obesity, has raised questions about appropriate prescribing, long-term safety, and equitable access. Authorities are monitoring how these drugs are being used across different care settings, including telehealth platforms and direct-to-consumer models. The challenge is to support innovation while maintaining clinical standards and patient protection.
Coverage policy is another area of active evolution. As evidence accumulates on the broader benefits of GLP-1 therapies, pressure is building to expand reimbursement for obesity indications. At the same time, the high cost of these drugs creates tension within healthcare systems, particularly in publicly funded programs. Policymakers must balance the potential for long-term cost savings against immediate budget constraints. There is also a conceptual shift underway. Obesity is increasingly framed as part of a continuum of metabolic disease, rather than as a separate condition. This reframing has implications for how GLP-1 therapies are positioned, potentially reducing the distinction between diabetes and weight loss indications over time. If obesity is fully integrated into metabolic care models, the current divide in coverage and treatment pathways may begin to narrow.
At the same time, new therapeutic approaches are emerging. Combination therapies, novel receptor targets, and alternative delivery systems are in development, aiming to improve efficacy, tolerability, and convenience. These innovations may further reshape the landscape, introducing new options and new complexities.
For pharmacies and providers, staying aligned with these changes requires continuous adaptation. Guidelines are evolving, formularies are shifting, and patient expectations are rising. The system is not stabilizing; it is accelerating.
Conclusion
GLP-1 receptor agonists now operate across two distinct but interconnected systems. In diabetes care, they remain part of a structured, guideline-driven approach focused on glycemic control and long-term complication prevention. In obesity care, they represent a rapidly expanding therapeutic frontier, centered on weight reduction, metabolic health, and patient-driven demand. The divergence between these systems is not merely clinical. It is reflected in access, prescribing authority, dosing strategies, patient expectations, and pharmacy operations. The same drug can be widely available in one context and difficult to obtain in another. It can be prescribed within a tightly controlled framework or through a decentralized network of providers. It can be viewed as essential therapy or as an optional intervention, depending on indication.
For patients, this means navigating a more complex treatment landscape, where outcomes depend not only on the drug itself but on the system surrounding it. For pharmacies, it means adapting to new workflows, new risks, and a more central role in ensuring safe use.
Looking ahead, there is potential for convergence. As obesity becomes more firmly recognized as a chronic metabolic disease, the gap between diabetes and weight loss treatment pathways may narrow. Coverage may expand, prescribing may standardize, and clinical frameworks may align.
For now, however, the split remains. One class of drugs, two systems of care, and a healthcare landscape that is still adjusting to the implications.